

Editor’s Note:
The Case Challenge series includes difficult-to-diagnose conditions, some of which are not frequently encountered by most clinicians, but are nonetheless important to accurately recognize. Test your diagnostic and treatment skills using the following patient scenario and corresponding questions. If you have a case that you would like to suggest for a future Case Challenge, please email us at ccsuggestions@medscape.com with the subject line “Case Challenge Suggestion.” We look forward to hearing from you.
Background
A 64-year-old woman presents to her family physician’s office with worsening groin and hip pain. She reports that she woke up one morning with pain in the proximal hamstring muscles of both thighs. A few days earlier, she had been gardening but recalls no other possible cause of these new symptoms. Over the next several days, the pain spread over both greater trochanters and into both groins. The pain worsened, waking her at night.
The pain is worse in the mornings but persists to some extent all day. She is unable to sit for long periods and must get up and move around. Similarly, she can drive only 30 miles before having to stop, get out of the car, and walk around. The pain makes it difficult for her to walk uphill or go upstairs.
Previously, the patient’s health was excellent. She takes no prescribed medications. She reports that she had a hysterectomy for dysfunctional uterine bleeding without complications. She has never smoked cigarettes or used illicit drugs, and she drinks one glass of wine on most days. Her family history is unremarkable.
Physical Examination and Workup
The patient’s vital signs, including temperature, are normal. Examination reveals marked tenderness over the ischial tuberosities, greater trochanters, both groins, and the symphysis pubis. Range of motion of both hips is limited and painful. No skin lesions are detected. The patient has no symptoms in her hands, and examination shows that the distal joints are normal. No tenderness over the scalp, face, or spine is noted. The eye examination is normal.
The results of blood tests, specifically the erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) level, are normal. The rheumatoid factor titer is negative. A radiograph of both hips is normal.
A nonsteroidal anti-inflammatory drug is prescribed (ibuprofen 200 mg three times a day) but the pain and disability persist. A few weeks later, the patient develops pain and stiffness of both shoulders. She is unable to elevate her arms beyond 90 degrees and has difficulty brushing her hair, fastening her bra at her back, and getting dressed.
She returns to her physician’s office. Examination confirms the loss of range of motion of the shoulders. Tenderness on the anterior and posterior aspects of each shoulder is noted.
Blood tests are repeated. On this occasion, the ESR is elevated, but the rheumatoid factor titer remains negative.
Discussion
Polymyalgia rheumatica (PMR) affects adults aged 50 years and older, and incidence rises progressively with age.[1] It is more common in women.[2] The cause is unknown, but synovitis in proximal joints and periarticular structures has been identified.
The symptoms and physical findings of polymyalgia rheumatica are nonspecific. Joint pain and stiffness are common complaints. A typical patient with PMR has acute-onset bilateral shoulder pain with morning stiffness. The shoulder girdle is affected in up to 95% of patients; the pelvic girdle and neck are also commonly involved. PMR may affect the knees and wrists, often asymmetrically, but the feet are usually spared.[3] More distal symptoms are present in about half of patients with PMR. Constitutional symptoms such as fatigue, low-grade fever, and weight loss are common. Active joint range of motion may be restricted, without observable joint inflammation or weakness.
There are no pathognomonic findings that can confirm the diagnosis, but a dramatic response to glucocorticoids is characteristic of PMR, and improvement is usually observed within 24-72 hours.
A positive temporal artery biopsy strongly suggests giant cell arteritis (GCA), not PMR. Subacromial bursitis is also seen in rotator cuff disease and calcium pyrophosphate deposition disease; no single imaging finding confirms PMR. Rheumatoid factor and anti-CCP seronegativity helps exclude rheumatoid arthritis but does not confirm PMR. ESR elevation is nonspecific and neither confirms PMR nor excludes it; this patient’s ESR was normal at her initial visit.
The diagnosis is based on the patient’s history, physical examination, and laboratory findings. No specific laboratory test exists for PMR. The ESR and CRP level are typically elevated in patients with PMR, but a normal ESR does not exclude the diagnosis.[4] The results of other laboratory tests, such as a complete blood cell count, liver function tests, and renal function tests, are usually normal. There are no disease-specific symptoms or laboratory markers for PMR.
Both ultrasonography and MRI can demonstrate synovitis of the subacromial bursa, glenohumeral joint, biceps tendon, interspinous region, hip joint, ischial tuberosity, and greater trochanter. MRI is more specific, with less interobserver variation, than ultrasonography.[5]
A relatively recent development in the imaging of PMR is the use of 2-deoxy-2-[18F]fluoro-D-glucose ([18F]FDG) PET combined with low-dose CT ([18F]FDG-PET/CT). This technique can evaluate all joints and extra-articular structures that might be affected in a patient with the disease.[6] Figure 1 shows an example of this imaging type in a patient with PMR.
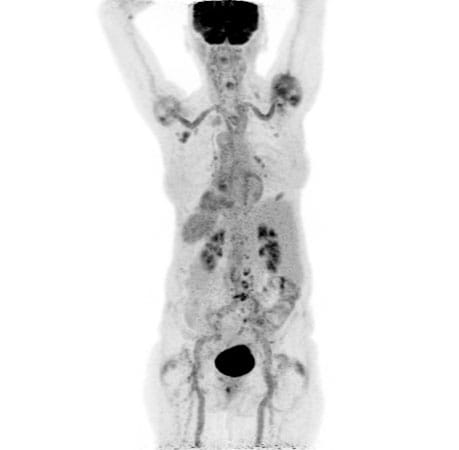
Figure 1. FDG PET showing inflammation around the shoulder muscles and lower spine, consistent with PMR, along with inflammation in the walls of major arteries, consistent with GCA. See Editor’s Note.
The differential diagnosis of PMR includes osteoarthritis, systemic infection, fibromyalgia, systemic lupus erythematosus (SLE), rheumatoid arthritis, and seronegative spondyloarthropathy (SpA).
In middle-aged patients, the most common cause of joint pain is osteoarthritis. Among those older than 45 years, osteoarthritis is more common in women than in men. The pain of osteoarthritic joints can be severe and disabling. After the knee, the hip is the joint most often affected by osteoarthritis. Clinically, hip osteoarthritis is characterized by groin pain, joint stiffness, and loss of function. Radiographs are abnormal and show decreased joint space, marginal osteophytes, subchondral cysts, and subchondral sclerosis. Results of blood tests are normal.[7]
Systemic infection can cause weakness, joint pain, and disability, but these are minor complaints compared with the other findings of general malaise, fever, tachycardia, and usually a source of infection. Blood test results are abnormal; both the ESR and the white blood cell count are elevated.
Fibromyalgia is characterized by chronic widespread pain throughout the body, fatigue, sleep problems, and cognitive difficulties. The pain can affect any part of the body, but it is most common in the neck, shoulders, back, hips, and legs. Typically, physical examination reveals tender points. Blood test results and radiographs are normal.
Joint pain is a common symptom of SLE, which most often affects the more peripheral joints of the hands, wrists, and knees. Affected joints may be swollen and warm as well as tender. A butterfly-shaped rash on the cheeks and nose is a classic symptom of SLE, and fatigue is also common. Laboratory test results are abnormal in patients with SLE. The ESR and CRP level are elevated, and anemia is common. Antinuclear antibody is positive in up to 99% of patients, and anti–double-stranded DNA antibody tests may be positive. Joint radiographs may be normal.
Chronic joint pain, usually symmetrical, is the hallmark of rheumatoid arthritis. As in SLE, the joints most commonly affected are those of the digits and the wrists, knees, and feet. On examination, affected joints are tender, swollen, and stiff. Not only are the ESR and CRP level high, but tests for anti-cyclic citrullinated peptide antibody and rheumatoid factor may be positive as well. Until erosive disease or secondary osteoarthritic changes develop, radiographs of the larger joints may remain normal or show juxta-articular osteoporosis.
Seronegative spondyloarthropathies are a group of chronic inflammatory diseases that affect the spine and other joints. Symptoms of SpA include back pain that is worse in the morning and improves with activity; arthritis of the hips, knees, and feet; uveitis; and inflammatory bowel disease, such as Crohn’s disease or ulcerative colitis. Blood tests for inflammatory markers, such as the CRP level and ESR, are elevated. A human leukocyte antigen B27 test may be positive. The rheumatoid factor test is negative. The diagnosis of SpA is made on the basis of the combination of clinical symptoms, examination findings, laboratory tests, and imaging studies. No single test can definitively diagnose SpA.
Giant cell arteritis and PMR are overlapping inflammatory rheumatic disorders. Up to 20%-25% of patients with newly diagnosed PMR may have subclinical GCA detectable via imaging, and symptomatic GCA develops in 10%-21% of patients with PMR.[8] Giant cell arteritis may cause headache, vision changes, and jaw claudication. Examination shows temporal artery tenderness. A dreaded complication is permanent vision loss. Patients with PMR and subclinical GCA have approximately a fourfold higher relapse rate than those with isolated PMR.[9]
For the treatment of PMR, EULAR/ACR guideline recommendations advise initiating prednisone at 12.5-25 mg/day, tapering to 10 mg/day within 4-8 weeks, then reducing by 1 mg every 4 weeks, with a goal of glucocorticoid discontinuation guided by symptoms and inflammatory markers. Total treatment duration is typically 12-24 months.[4]
In the patient in this case, prednisone 20 mg/d was prescribed. She noticed a dramatic improvement within 48 hours. Six weeks later, the prednisone dosage was reduced to 10 mg/d, without any increase in symptoms.
Follow-up
Symptoms, blood test results, and the possibility of GCA will be assessed regularly, at least every 4-8 weeks initially, then every 3 months once stable.[4] Long-term corticosteroid use can have adverse effects, including weight gain, loss of bone density, high blood pressure, diabetes, and cataracts, which must be monitored. Per 2022 ACR guidelines on glucocorticoid-induced osteoporosis, patients initiating long-term glucocorticoid therapy should receive fracture risk stratification using FRAX, bone mineral density testing, and, in most cases, calcium, vitamin D, and bisphosphonate therapy.[10]
If a patient does not respond sufficiently to corticosteroids, the addition of methotrexate can be considered. In addition, sarilumab, an IL-6 receptor antagonist, was approved by the FDA in February 2023 as the first biologic indicated for PMR in adults who have had an inadequate response to corticosteroids or cannot tolerate corticosteroid taper.[11] Tocilizumab, another IL-6 receptor antagonist, has also shown glucocorticoid-sparing benefit in retrospective and small randomized studies, although it lacks an FDA indication for PMR.[12]
Prognosis
The overall prognosis of PMR is difficult to determine, but follow-up studies report that 25%-40% of patients continue to take corticosteroids 5 years after diagnosis. Older patients are more likely than younger ones to remain on steroid therapy.[13]
Editor’s Note: Figure 1 is from a different patient with a similar condition.
Editor’s Note: This article was created using several editorial tools, including generative AI models, as part of the process. Human review and editing of this content were performed prior to publication.
Comments are closed.